RegenHRT: A More Precise Approach to Hormone Therapy

Why traditional hormone therapy often falls short, and how a more precise, physician-guided approach can improve both symptoms and long-term health.
- Many women today fall into two groups: those who have never taken hormone therapy and could still benefit, and those who are already on HRT but may not be getting the full benefits.
- The question is no longer simply whether hormone therapy should be used, but whether treatment restores hormones to physiologic levels and is monitored appropriately.
- In many parts of the world, hormone therapy is used not only for symptom relief, but to help prevent long-term conditions such as osteoporosis.
- RegenHRT™ was designed to bridge that gap by combining individualized treatment planning, therapeutic hormone targets, and ongoing monitoring.
Understanding menopause as a hormone deficiency state
Menopause and perimenopause are best understood as hormone deficiency states.
Our bodies rely on hormonal signaling for countless functions—from highly specialized processes like reproduction to basic functions such as metabolism, bone maintenance, sleep regulation, and brain function. Some of our hormone levels gradually drop with age, fading slowly over time.
Menopause is different. Instead of a slow fade, it’s a relatively abrupt shutdown of ovarian hormone production. Within a fairly short period of time, estrogen and progesterone levels fall dramatically.
For decades, a woman’s tissues have relied on those hormones as daily signals. When those signals disappear, the tissues that relied on them don’t function as well. Bone loss accelerates, metabolic regulation shifts, sleep and temperature control become unstable, and many other changes we associate with menopause – and aging more broadly – occur.
When we replace those missing hormones carefully, not only do women feel better, they also are much less likely to develop conditions and risks they otherwise would if those deficiencies were allowed to continue. That’s why the head of the FDA said,
“There may be no other medication in the modern era that can improve the health outcomes of women… (more) than hormone replacement therapy.” Dr. Marty Makary, MD, MPH, FDA Commissioner, Nov. 10 2025
As simple and logical as it sounds to simply replace these needed hormones, only a few percent of women have taken menopausal hormone replacement since 2002 (see the How Did We Even Get Here? section below). For years the conversation around hormone replacement therapy (HRT) has been black and white: “should I or shouldn’t I?” But now most health authorities have reversed position and agree that hormone replacement is, for the most part, an important treatment that almost all women should consider. The real issues arising are about how HRT is prescribed and managed. Even when they’re already taking hormone therapy, the treatment women receive often isn’t optimized for symptom relief, long‑term health, or disease prevention.
Why many women are not getting the full benefit of hormone therapy
When it comes to hormone therapy in our clinics, we usually see two types of women: those who have never seriously considered hormone therapy, and those who are already on it but may not be getting the most out of their current treatment.
Many in the first group thought they were too young, too old, or may have been scared off by breast cancer or other fears. Others simply heard that menopause symptoms are something they just have to live with. Most of these women can still benefit from hormone replacement, sometimes dramatically.
The second group is becoming increasingly common: women who are already taking hormone therapy and believe they are ahead of the curve. Yet many of these patients still struggle with fatigue, brain fog, poor sleep, low libido, or persistent hot flashes. In many cases the issue is not whether hormone therapy is being used, but how it is being prescribed. Often the doses are just enough to relieve a few symptoms, but too low to give the full benefits for prevention of osteoporosis, heart health, and more.
Not only are typical estrogen doses too low to reach therapeutic levels, hormone levels usually aren’t even measured, and testosterone—an important hormone for women—is rarely discussed. As a result, many women who believe they are receiving modern hormone therapy are actually receiving an overly cautious version of treatment that reflects older fears rather than current evidence.
How hormone therapy became misunderstood in the United States
For almost 25 years, hormone therapy carried a powerful stigma following early misinterpretations of the 2002 WHI study. That study used a combination of horse-derived estrogens and synthetic progestins (very different from what is typically prescribed today), and showed small increases in breast cancer risk. That unexpected finding caused what has been described as a national panic among women using HRT for menopause. Almost overnight, millions of women stopped treatment.
Following the overreaction to the WHI study, physicians and patients alike avoided hormone replacement entirely for years, especially in the US. Even after later research debunked the WHI and showed that hormone therapy actually provides major health benefits, recommendations in the US discouraged HRT for all but the most severe menopausal symptoms. Most US medical societies continued to ignore the disease prevention benefit that became well-researched and known in the 2010’s.
This led to the “lowest effective dose for the shortest time” standard in the US for hormone replacement. The belief was that if women were really, really miserable with hot flashes, one could reasonably prescribe a small amount of estradiol to “get them through” until they could tolerate their menopause symptoms. There was no thought of what the best dose would be to rebuild bone, or to protect the heart and blood vessels as estrogen has been shown to do. While well‑intentioned, these low doses often leave patients with only partial symptom relief and hormone levels well below physiologic, disease preventing ranges. This low-dose, short duration treatment dogma still exists today, especially in American medicine.
This is very different from the medical experience in the rest of the world. In England, Australia, and many Western European countries, recognizing flaws in the WHI study and the many health benefits of HRT happened much more quickly. For physicians and the general public there, the question of whether or not hormone replacement is generally a good thing was answered long ago. Today, discussions in those countries focus on how to achieve the best levels for both symptom relief and disease prevention. Not only are estrogen and progesterone routinely recommended, testosterone is widely prescribed for menopausal women as well.
Five Signs Your Hormone Therapy May Not Be Optimized
Many women assume that once they start hormone therapy they are receiving the full benefits of treatment. In reality, some patients remain on doses that relieve a few symptoms but never restore hormone levels to physiologic ranges. Warning signs may include:
- Never having hormone levels measured
- Experiencing only partial symptom improvement
- Never discussing testosterone therapy
- Focusing only on symptoms rather than hormone levels
- Staying on the same treatment and dose for years without reassessment
A surprising number of patients coming to our clinic fall into this category. They’re already prescribed hormone therapy elsewhere, but typically the dose is simply too low to restore physiologic hormone levels or other key hormones like testosterone were never considered. Patients often notice improvements they didn’t think were possible once we optimize their treatment regimen.
That gap between optimal hormone replacement and what is actually being delivered to women in the US is what led us to develop RegenHRT™, a structured clinical system designed to deliver hormone therapy in a more precise and physiologically informed way.
RegenHRT, a more precise approach to hormone therapy
How RegenHRT™ Works
RegenHRT™ begins with baseline testing. Symptoms, medical history, and laboratory values are reviewed in order to understand where hormone levels are starting. This evaluation provides the physiologic context needed to design an effective treatment plan.
A personalized hormone plan is then created. Age, body composition, previous treatments, and clinical variables are considered to determine what hormones may be missing and which combination is most likely to restore physiologic balance. Estradiol, progesterone, testosterone, or combinations of these hormones may be used depending on the patient’s physiology and goals.
Dosing follows a clinical framework designed to restore therapeutic hormone levels rather than relying solely on trial‑and‑error symptom relief. Finally, symptoms, laboratory values, and clinical response are monitored so therapy can evolve as the body changes.
Why Hormone Testing Matters
Who treats high blood pressure without checking your blood pressure? Does anyone prescribe cholesterol medication without measuring a cholesterol level? Hormone therapy should follow the same medical logic. Measuring hormone levels is the only way to determine whether treatment is actually reaching therapeutic ranges. Of course it’s important to feel better, which can happen at low doses; but our patients are happier knowing their bones aren’t dissolving too – and that takes a therapeutic dose.
What Are Therapeutic Estradiol Levels?
Research over several decades has shown that estradiol levels influence multiple physiologic systems including bone metabolism, cardiovascular function, metabolic regulation, and brain health. One important example is osteoporosis. Studies examining bone turnover show that estradiol levels below roughly 30–40 pg/mL fail to adequately suppress bone resorption after menopause. This is the common level women in the US achieve with HRT – it’s enough to calm hot flashes, but not enough to adequately protect bones.
Levels closer to approximately 60–100 pg/mL are associated with normal physiologic estrogen activity in many tissues. At those levels, studies show improved blood vessel function, slower buildup of cholesterol plaques, improved skin, vaginal, and bladder tissues, and of course reversal of bone loss. However, many – even most – women receiving hormone therapy remain below these ranges, again probably due to the outdated philosophy of “lowest dose, shortest time.”
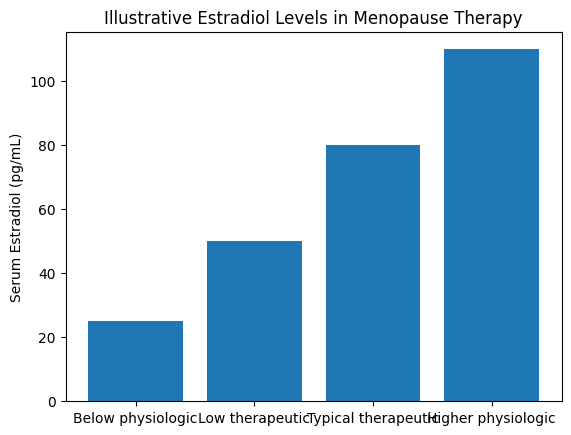
Figure 1. Illustrative estradiol levels in menopause and hormone therapy.
Why delivery method and monitoring both matter
Blood level studies of estradiol patches demonstrate why testing matters. With hormone patches, estradiol levels often rise soon after patch placement and then gradually decline over several days. Studies in the UK and Australia have shown most women on estrogen patches don’t reach therapeutic levels. Even on the highest dose patch, 25% still don’t reach ideal levels. But we shouldn’t just point out patches – many compounded topical creams don’t reach therapeutic levels either. In the end, it’s more a problem of monitoring and treatment guidance than it is with the drug delivery itself.
Unless we’re talking about estrogen pills. That’s the one method of replacing estrogen that’s actually been proven to increase risk – of blood clots, specifically. It has to do with the way estradiol changes when it’s absorbed through the intestines (as opposed to being absorbed through or beneath the skin as with patches, creams, and pellets). When women swallow estrogen tablets, the hormone is absorbed through the small intestine and immediately flows through the liver, which responds by producing more blood clotting factors. Women taking oral estrogen have double the risk of developing blood clots compared to women who aren’t taking estrogen pills.
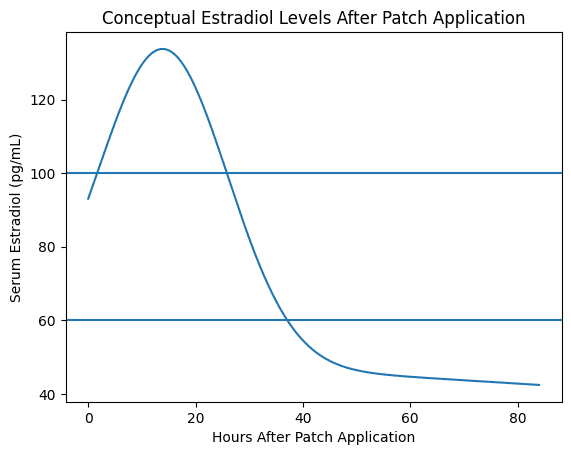
Figure 2. Conceptual representation of estradiol levels after transdermal patch application.
The role of testosterone in women’s health
Although commonly associated with men, testosterone is also an important hormone in women. Women actually make more testosterone in their lifetimes than they do estrogen. Even after menopause, the ovaries continue to produce small amounts of testosterone. It influences sexual desire, energy levels, muscle mass, motivation, and aspects of cognitive function. Yet testosterone therapy is rarely discussed during menopause care. With RegenHRT, testosterone is almost always part of the program.
Most studies on testosterone replacement in women are focused on libido. Many research studies have shown clear improvement in sex drive when women’s testosterone levels are far below their youthful peak. In fact, that is the official indication for its use in women in the UK and Europe (the US FDA, on the other hand, has never approved testosterone replacement in women).
Despite the lack of FDA approval in the US, one of the most important clearly proven benefits of testosterone replacement in women is osteoporosis prevention. Most of us know that estrogen is important to maintain and build healthy bones, but very few know that about testosterone. Studies on menopausal women show that replacing testosterone to physiologic levels improves bone density 50% more than estrogen replacement alone. In other words, it’s not a replacement for estrogen, but it does enhance estrogen’s bone protective effects – by a lot!
Interestingly, one of the problems with testosterone replacement in women is the opposite of the estrogen replacement problem. Whereas estrogen is commonly underdosed, testosterone in women is often dosed too high, leading to what are known as supra physiologic levels – much higher than what women naturally produce at their peak. With testosterone, women can definitely have “too much of a good thing.” They can experience side effects including hair loss on the scalp, as well as excessive hair growth elsewhere (chin, upper lip, body). There are plenty of studies showing the benefits of supplementing women’s testosterone to normal, female physiologic levels; there is no evidence that abnormally high levels have any benefit.
This reinforces the major theme of this blog: the importance of testing and monitoring hormone replacement to ensure the best outcomes. The goal of treating any deficiency is to replace it to normal levels – not to boost it unnaturally without clear purpose.
Common Mistakes in Hormone Therapy
Hormone therapy has evolved significantly over the past two decades, but the way it is often prescribed has not always kept pace with the science. Common issues include dosing based only on symptom relief, fear‑driven underdosing that reflects outdated concerns, and the absence of testosterone discussion in many treatment plans.
The bottom line, a more thoughtful approach to hormone therapy
The modern conversation about hormone therapy is no longer simply about whether hormones are used. The more meaningful question is whether treatment restores hormones to physiologic levels and is monitored appropriately. RegenHRT™ was developed to provide a structured system for individualized hormone therapy combining personalized treatment planning, therapeutic hormone targets, and ongoing monitoring.
If you’re considering hormone therapy, or are already on treatment but not feeling your best, a more structured approach may make a meaningful difference.
📍 You can find personalized hormone therapy for perimenopause and menopause at RegenCen in:
- Northern Michigan: Petoskey, Harbor Springs, Traverse City, Suttons Bay
- Southeast Michigan: Bloomfield Hills, Ann Arbor, Fenton, Chelsea, East Lansing
- West Michigan: Grand Rapids, East Grand Rapids
- Southwest Florida: Naples, North Naples, Marco Island, Boca Grande, Sarasota
- Southeast Florida: Palm Beach, Hobe Sound, Vero Beach, Wellington
- Central Florida: Winter Park, Lake Mary
- Northeast Florida: Atlantic Beach
- South Carolina: Bluffton
Schedule a consultation at RegenCen near you in Michigan, Florida, or South Carolina (opening May 2026!) to learn more about RegenHRT.
